
Two conditions. Millions of women. Decades of suffering. Polycystic Ovary Syndrome (PCOS) and Endometriosis are two of the most common gynecological disorders affecting women worldwide—yet both remain profoundly misunderstood, underdiagnosed, and frequently dismissed. Despite affecting an estimated 10% of women of reproductive age (PCOS) and another 10% (endometriosis), the journey to diagnosis often takes years, punctuated by countless medical visits where pain is minimized, symptoms are normalized, and women are sent home to “manage” what society has taught them to endure.
The Conditions: What They Are and Why They Matter
Though both affect the reproductive system, PCOS and endometriosis are distinct conditions with different mechanisms, symptoms, and impacts.
PCOS (Polycystic Ovary Syndrome) is a hormonal disorder characterized by:
Irregular or absent menstrual periods
Elevated levels of androgens (male hormones), which can cause excess facial and body hair, acne, and male-pattern baldness
Polycystic ovaries visible on ultrasound
Metabolic effects including insulin resistance, weight gain, and increased risk of type 2 diabetes
Fertility challenges due to irregular ovulation
Endometriosis is a condition where tissue similar to the uterine lining grows outside the uterus—on ovaries, fallopian tubes, bowel, and other pelvic structures. This misplaced tissue responds to hormonal cycles, bleeding and inflaming each month with no way to exit the body, leading to:
Severe, debilitating pelvic pain, especially during menstruation
Pain during or after intercourse
Pain with bowel movements or urination
Heavy menstrual bleeding
Infertility
Chronic fatigue
Despite their differences, both conditions share a common thread: women suffer in silence while medicine catches up.
The Diagnostic Odyssey: Why It Takes So Long
The average time to diagnosis for endometriosis is 7–10 years. For PCOS, it is often 2–4 years. This delay is not due to rarity—it is due to a culture that has normalized women’s pain.
Common Barriers to Diagnosis:
Normalization of Suffering: Young women are told that painful periods are “just part of being a woman.” Cramps that leave them unable to function are dismissed as normal. This messaging begins in adolescence and continues through adulthood.
Symptom Overlap and Misdiagnosis: Both conditions share symptoms with irritable bowel syndrome (IBS), pelvic inflammatory disease, and other disorders. Without proper investigation, women are often misdiagnosed and treated for the wrong condition for years.
Invasive Diagnostic Procedures: Endometriosis can only be definitively diagnosed through laparoscopy—a surgical procedure. This creates a high barrier to diagnosis, with many women hesitant or unable to access surgical evaluation.
Gender Bias in Healthcare: Numerous studies have shown that women’s pain is taken less seriously than men’s. Women are more likely to be told their pain is “anxiety” or “stress” and are less likely to receive pain medication or further investigation.
Lack of Specialist Knowledge: Many general practitioners have limited training in these conditions, leading to referrals that never happen or treatment that addresses symptoms without investigating root causes.
The Hidden Toll: Beyond Physical Pain
The impact of these conditions extends far beyond physical symptoms:
Fertility and Family Planning: Both conditions are leading causes of infertility. For women who desire children, this adds profound emotional weight to an already difficult diagnosis.
Mental Health: Women with PCOS and endometriosis have significantly higher rates of depression, anxiety, and eating disorders. The combination of chronic pain, body image concerns (particularly with PCOS-related hair growth and weight changes), and fertility struggles takes a severe psychological toll.
Career and Education: Missed workdays, reduced productivity, and the need for frequent medical appointments affect professional trajectories. Women with severe endometriosis lose an average of 11 hours of work per week.
Relationships: Pain during intercourse, fatigue, and the emotional burden of chronic illness strain intimate relationships. Many women report feeling “broken” or inadequate as partners.
Why the Confusion Between PCOS and Endometriosis?
The conditions are frequently conflated in public discourse, but they are fundamentally different:
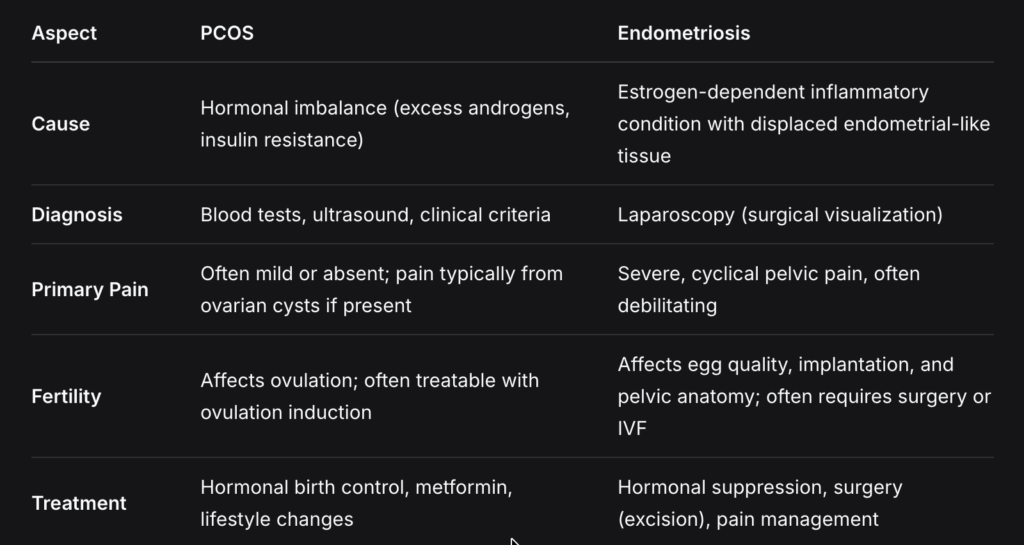
A woman can have both conditions simultaneously, further complicating diagnosis and treatment.
The Path Forward: What Needs to Change
For Healthcare Systems:
Improved Medical Education: Medical schools must dedicate more time to gynecological conditions beyond obstetrics. Recognizing PCOS and endometriosis as common, serious conditions should be standard.
Shorter Diagnostic Pathways: Protocols that reduce time to specialist referral, rather than months of failed treatments for misdiagnosed conditions.
Multidisciplinary Care: Access to gynecologists, pain specialists, nutritionists, mental health providers, and fertility specialists working together.
For Women and Individuals:
Track Your Symptoms: Document pain levels, cycle irregularities, and associated symptoms. Data is power in medical appointments.
Advocate Persistently: If a provider dismisses your pain, seek a second opinion. You are not “being difficult”—you are advocating for your health.
Find Specialists: Seek out gynecologists who specialize in PCOS or endometriosis. Generalists may lack the depth of knowledge these conditions require.
Connect with Community: Support groups (online and in-person) provide validation, practical advice, and a reminder that you are not alone.
For All of Us:
Believe Women: When a woman describes pain, believe her. This simple shift would transform diagnostic timelines.
Stop Normalizing Suffering: Painful, debilitating periods are not “normal.” Speak up when you hear this messaging.
Support Research: Both conditions remain underfunded relative to their prevalence. Advocate for research that explores causes, treatments, and potential cures.
The Bottom Line
PCOS and endometriosis are not rare. They are not niche. They are not “just bad periods.” They are chronic, complex conditions that affect tens of millions of women worldwide—and the suffering they cause has been minimized for far too long.
The misunderstanding of women’s pain is not a failure of individual doctors alone. It is a systemic failure rooted in a culture that has historically treated women’s bodies as mysterious, their pain as exaggerated, and their suffering as something to be endured. The path to better outcomes begins with naming this failure, demanding better, and refusing to accept “it’s normal” as an answer.
Your pain is real. Your experience is valid. And you deserve care that takes you seriously.
FAQ:
Q: Can you have both PCOS and endometriosis?
A: Yes. It is possible to have both conditions simultaneously, which can complicate diagnosis and treatment. Some studies suggest women with PCOS may have a slightly lower risk of endometriosis due to hormonal differences, but the conditions are not mutually exclusive.
Q: Is it possible to get pregnant with PCOS or endometriosis?
A: Yes, though fertility may be affected. Many women with PCOS conceive with ovulation induction medications. Women with endometriosis may conceive naturally or require surgical intervention or assisted reproductive technologies like IVF. Individual prognosis varies based on severity and other factors.
Q: Are there lifestyle changes that help?
A: For PCOS, lifestyle modifications including diet, exercise, and weight management can significantly improve symptoms and metabolic health. For endometriosis, anti-inflammatory diets, stress management, and pelvic floor therapy may help manage symptoms, though they do not eliminate the disease.
Q: How do I find a specialist?
A: Look for gynecologists who list PCOS or endometriosis as specialties. For endometriosis, seek surgeons who perform excision (removal) of endometrial lesions, not just ablation (burning). Online communities often maintain lists of recommended specialists. University-affiliated hospitals and specialized clinics are good starting points.
Q: Is there a cure?
A: Currently, there is no cure for either condition. PCOS is managed as a chronic condition through hormonal regulation and metabolic support. Endometriosis is managed through hormonal suppression, surgery, and pain management, though symptoms often recur without ongoing treatment. Research into both conditions is ongoing.















